Between the Medicare open enrollment period and the Exchanges opening up for enrollment in a few weeks, a lot of people will be making a lot of tough, and hard to fully describe choices for their health insurance. I, personally, have a much easier choice set but I want to go through my decision process on how I chose the insurance for 2019 for my family last night.
-
- Grab a beer (I recommend 21st Amendment Blood Orange)
- List probable future medical utilization
- Flu shots
- 2 Pediatric well child (docs @ Duke)
- Several PCP visits for school age crud
- 1 or 2 adult wellness visits (my doc is @ Duke)
- 1 or 2 urgent care visits for random stuff
- 1 OB-Gyn well visit (no relationship established)
- Possible surgery to clean up a broken ankle if it does not heal right
- Expected Pharmacy Utilization
- Asthma crisis medications (generic nebulizer and brand name blue inhaler)
- Asthma maintenance medications (brand name orange inhaler)
- Confirm Pharmacy benefit is the same across all plans
- Eliminate the nationwide PPO and the North Carolina wide HMO network plans as they are too expensive. The less expensive narrow network choices are built around Duke owned facilities. If one of us has something weird, we’re likely going to Duke anyways as Duke handles a good chunk of the complex/weird cases.
- Choices are now restricted to a no deductible/co-pay only Plan A. It has a higher premium coming out of my paycheck compared to Plan B which has a $600 deductible/$2,000 individual maximum out of pocket or $1,800 family deductible/$6,000 family maximum out of pocket plan.
Before I go further, I just want to state that this is damn good insurance. The low AV plan is low platinum level coverage and the no deductible plan is high platinum coverage. This is damn good coverage.
I had to figure out which would cost the family the least. My son’s asthma medications are a constant cost, so they are analytically irrelevant. My wife has a broken ankle. So far she is healing well. The orthopedic surgeon has told her that in similar cases, he frequently will need to go in and install screws/plates if everything does not heal up right after several months of light activity and supportive stabilization. This is our big question mark.
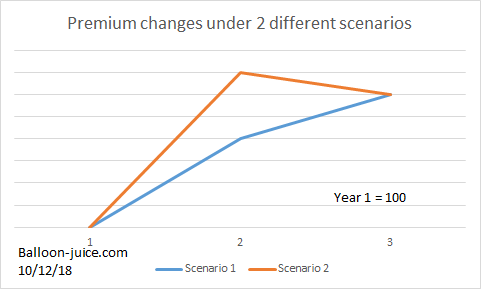
Assuming that she needs surgery, we figure it is at at least a $5,000 operation with at least a dozen physical therapy sessions afterwards. Under Plan A we would pay a $600 hospital admission co-pay and then $240 in PT co-pays. Under Plan B, she would max out her deductible of $600 and run up most of her out of pocket limit through PT co-pays and coinsurance for the surgery.
If she needs surgery, Plan A is the better choice as the higher monthly premiums buy out the deductible and it has much lower co-pays. Conditional on my wife needing ankle surgery, Plan A has us coming out ahead by about $1,000 for the year. If she does not need surgery, Plan B is a better value by $1,500 or so for the year.
We don’t know if she needs surgery yet. We don’t have a good way to estimate our probabilities beyond the vague information from her orthopedist that he “frequently” needs to go in. I don’t know what “frequently” means. Is it 20% of the time, or 50% of the time or does he slice and dice 85% of the time? I don’t know.
At this point in the analysis, it was no longer analytical. It had to become a discussion about tolerances and values. I grabbed a beer for my wife, and she turned on The Good Place before we talked about our risk tolerances and our ability to take a hit on bad outcomes arrived through a good process. This is mostly a values questions. It reflects our risk tolerance at this point in our lives is not a perfectly rational loss/reward frontier. We decided that we would stick with Plan B as we can afford an incremental $1,000 hit if she needs surgery although we’ll grumble about it. But we would regret the extra $1,500 in spending if she does not need surgery.
This is how we made our insurance decision for next year. And this was a very easy set of choices. We started with four choices with significant elements constant across all possibilities (the prescription drug benefit). We eliminated from consideration the two expensive broad network options. We then primarily focused on one possibility. We excluded from consideration unusual and very high cost events as both plans will be good enough for a cancer diagnosis or similar events. And even with that simplification, we’re gambling on imperfect information on what we need. I think we will have satisfied minimal criteria but I know we are not optimizing our decision making.
This is the easy case.
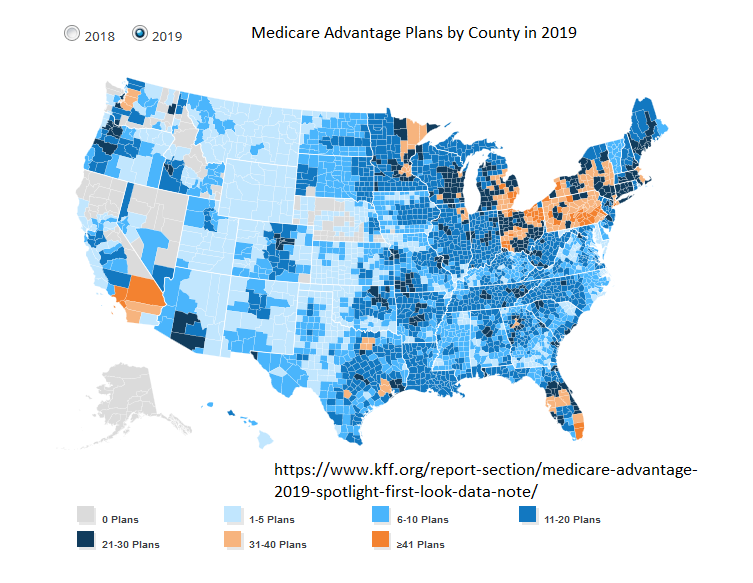
Some Medicare Advantage buyers will look at forty or more plans in 2019. Some ACA Exchange buyers will see over 100 plans offered in their county in 2018. The language used to described the same element will vary wildly between insurers and the prescription drug benefits will also have significant confusion introduced by variation. This is a tough choice. And it is a choice where I think most people need to go into the decision matrix knowing that they won’t get the optimal choice but if they lay out a series of minimally acceptable criteria, that they can get a good enough choice.