Market structure in revenue neutral risk adjustment should drive incremental coverage decisions.
Risk adjustment moves money to insurers that have a sicker than average population to cover. There are two flavors of risk adjustment financing that have very different incentive structures for coding. Widget risk adjustment like Medicare Advantage has a central payer (the federal government) that pays a fee for each qualified diagnosis any insurer submits on a claim. Revenue neutral risk adjustment has insurers with low population morbidity send money to insurers with higher than average medical burden. A dollar that Insurer A gains is a dollar that Insurer B loses. The ACA is risk adjusted in this manner. Some state Medicaid managed care programs like Pennsylvania, where I used to work and optimized the risk adjustment search system for UPMC for You, also have revenue neutral risk adjustment.
Widget risk adjustment leads to upcoding. Legitimate upcoding is the incentive for insurers to get their doctors to code everything that is medically defensible onto a claim. Medicare Advantage patients will have more diagnosis categories than identical fee for service Medicare patients. Medicare Advantage insurers will chase diagnosis codes that their data sets indicate should be credited but have not yet been credited. The decision structure for any given insurer is simple: Chase every diagnosis until the incremental revenue gain is outweighed by the chase, hassle and piss off the providers costs. It is not a strategic decision that has to incorporate other actors’ behaviors.
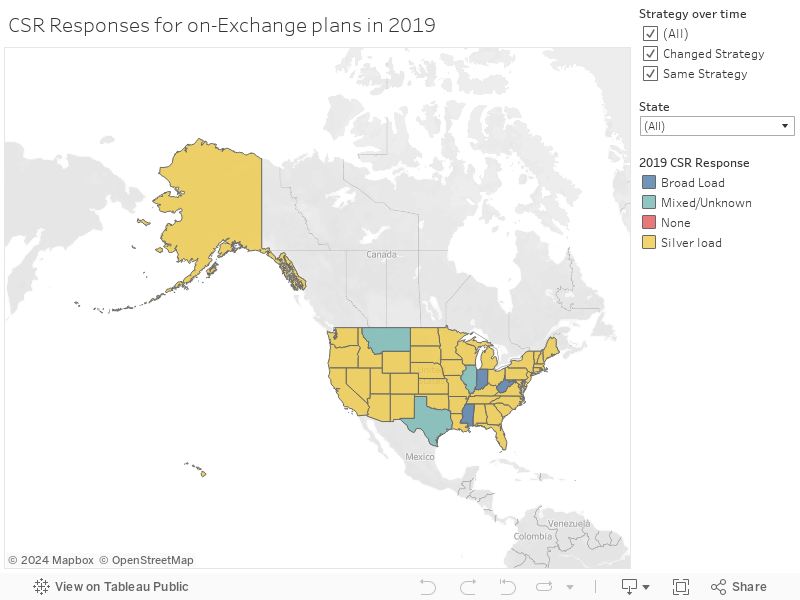
Revenue neutral risk adjustment can be a strategic decision depending on the market structure which will lead to very different chase incentives. The ACA risk adjusts the metal plans in the individual market by state.
An insurer that has a state wide monopoly has no incentive to care about coding as a revenue enhancement measure. Any coding concern should be relevant to either clinical treatment concerns, claims payment reasons or population health measures. There is no money to be made or lost by chasing risk adjustment points.
States that have two insurers have a wide range of incentives. If there is a split market with a single dominant insurer (Insurer A) and an insurer that has minimal market power/enrollment (Insurer B), Insurer A may be indifferent to chasing risk adjustment gains as the dollars at risk is a very small proportion of total revenue. The rewards and costs for Insurer A are low. Insurer B has strong incentives to optimize their risk adjustment. A $1,000,000 risk adjustment swing is merely an accounting error for Insurer A and a company existence event for Company B.
If there are two more more insurers with decent market share in a state, we get a red queen’s race. Insurers will have strong reasons to chase every defensible diagnosis ( and some that may not be defensible). It won’t add to their revenue but it will prevent a competitor from getting undeserved revenue. This is an expensive behind the scenes administrative arms race.
Why does this matter?
I think this is a good identification strategy for Hep-C dispensing incentives for insurers:
the ACA risk adjustment program is highly likely to overpay for Hep-C anti-viral prescriptions this year and next year due to list price reduction shocks. The price that insurers pay will be significantly below the prices used to determine risk-adjustment co-efficients.
I think that insurers will be seeing too large of a risk adjustment score for the dispensing of a Hep-C anti-viral prescription. Monopolistic insurers won’t have any risk adjustment incentives to change their behavior. Insurers that are overwhelmingly dominant in a state will have very weak incentives to change their behavior. Very small insurers will have bet the company incentives on increasing Hep-C prescriptions. Insurers (regardless of enrollment) in competitive states will have strong incentives to increase their Hep-C anti-viral cures.