The Center for Medicare and Medicaid Services recently released an audit study on the doctor and hospital directories that Medicare Advantage insurers are required to supply to members. Directories are supposed to tell insurance buyers what doctors and hospitals are in network, where those offices are located, how to contact those offices and whether or not the doctor is taking new patients from a particular insurer.
The results are abysmal.
The majority of the MAOs (28 out of 52) had between 30% and 60% inaccurate locations.Because MAO members rely on provider directories to locate an in-network provider, these inaccuracies could pose a significant access-to-care barrier.
Inaccuracies with the highest likelihood of preventing access to care were found in 41.7% of all locations.
A few thoughts. First, CMS is doing a damn good job of conducting effective oversight. Secondly, I spent several years at UPMC Health Plan working making their directory and provider information systems hum. I don’t think that it is ever possible to have a perfect directory. As soon as the TRUTH is validated, it will change. However there is a wide degree of errors. Table 6 in the report gives me hope and disgust at the same time.
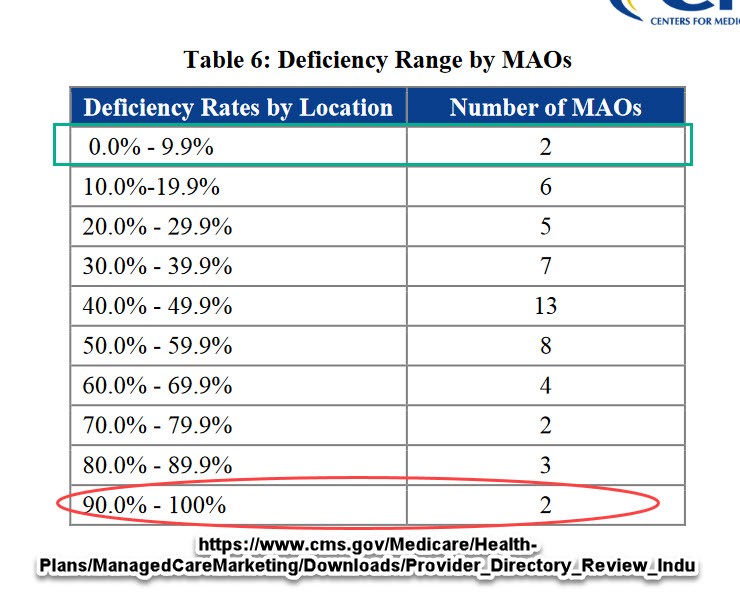 Two insurers showed that good to very good directories are possible. Two insurers make a complete farce out of the idea that people can rely on directories.
Two insurers showed that good to very good directories are possible. Two insurers make a complete farce out of the idea that people can rely on directories.
Getting a directory right or at least good enough with a low error rate that is quickly corrected requires time, money and insurer management give a damn.
The CMS report highlights some of the typical problems. The biggest drive of bad directories is that the data is stale and the insurers rely on provider self-report. Insurers see good provider information when they go over a doctor’s credentialing package. This package is needed for the doctor-insurer contract. It will contain licensing information, practice locations and contact information. After the contract is signed, the data might be reviewed in three to five years. Any updates usually happen because the provider reports something.
I firmly believe that any data element that does not drive provider payment will not produce timely, accurate nor complete provider data.
Insurers that want to get good directories need to spend money and give a damn. They need to actively check provider information against national databases. They need to audit at least a proportion of their provider universe on a consistent basis. They need to send out account representatives to verify addresses. When one of their employees goes by a soon to be knocked down strip mall on the way to a D-3 women’s soccer game he is about to referee, the insurer needs to update the address status of the large primary care office that was in the strip mall. All of this takes time and money.
Directories are still seen as mostly a cost-center and not a profit center. CMS or state regulators can increase the costs of bad directories either directly with fines or indirectly by removing stars, changing auto-assignment policies for Medicaid managed care or increasing the scrutiny of plans that need state approval. Giving a damn so that people know what the hell they are buying should be a minimal first step in an environment where we expect the individual buyer to assert market discipline on insurance premiums and medical costs in general.
 On the Road and In Your Backyard
On the Road and In Your Backyard
Barbara
Providers are paid electronically for the most part, and even if they are not, their payment address is often different from their service location. So the details necessary for payment diverge from location information. I think people can forgive changes in suite number that the provider forgot to provide to the payer. What’s harder to understand are situations where a provider maintains that there is no and never has been a contract. In some cases, they are wrong, because the contract might be through an intermediary and they don’t realize that contract meant that they had agreed to participate in the such and such network.
David Anderson
@Barbara: Yep, there is an acceptable level of error and an acceptable type of error (Suite numbers are the easiest ones to forgive).
PAR or Not PAR and New Patients/Not New Patients are big challenges in my mind.
dr. bloor
Almost makes me think that updating my CAQH profile every six months, which insurers have ready access to, isn’t worth the trouble.
As an aside, is there any data as to how many patients actually end up with a doc by using the directory? Most folks I know only use it as a last resort.
ETA: the only useful New Patients/Not New Patients solution I’ve seen is used by a referral service the missus subscribes to, in which they have to update every thirty days or so, or get tossed from the service.
boatboy_srq
True both in the sense that two are apparently entirely inaccurate and in the sense that only two out of fifty-two were able to be 90+% accurate.
Barbara
@dr. bloor: People don’t usually end up going to a doctor’s office and then finding the doctor doesn’t take their insurance. People have to call and make appointments, and are almost always asked who their insurer is and told whether they are in or out of network. The problem is that people choose plans based on the breadth and depth of provider networks, and they are not going to verify the status of every doctor in their area that they are checking to see is in the network. I can understand how the information becomes stale, but we’ve heard of situations where providers were simply sure that they had never been in the network, ever and could not imagine how their name showed up.
Fred Fnord
Doesn’t California have regulations regarding this? I seem to recall that if something is listed as in-network on an insurer’s site, then they are obligated to treat it as in network? And there may be another regulation about if a provider claims to be in-network but isn’t.
Aardvark Cheeselog
I recently had an adventure with Cigna’s provider directory, which based on my experience would score in the lower half of the pack. It was just stupefyingly bad. I went through 20 or so entries before I found a hit.
In my fantasy world, there’s a law that allows people being jerked around by the “customer service” branches of organizations that they do business with to bill such businesses for their time at about $200/hr, and if enough such invoices pile up, to slap a lien on the CEO’s private jet until they’re paid.
Chris Johnson
This is atrocious. Quit your industry, it doesn’t deserve you, in the least.
Barbara
@Chris Johnson: Seriously, you wouldn’t believe how stupefyingly complex this actually is. Part of the complexity is just the fact that too many things are too complex because of the fragmented nature of the system itself, but I would bet money the HMOs at the top of this chart are entities like Kaiser and GHP that provide services mostly through a single group of providers and that retain tight controls on authorizations for services outside that group. But those are the kinds of plans that many consumers don’t like, which dumps them into the world of an insurer that might have hundreds of agreements, and some providers participate for commercial, but not Medicare and on and on. I bet that accounts for many of the mistakes. They have a contract, just not one that includes Medicare.
David Anderson
@Barbara: And as a side layer of complexity, some providers will have a Medicare Advantage HMO contract with Insurer X but not the Medicare Advantage PPO contract with Insurer X or vice versa.
One of the big challenges we had on Exchange directories is that one of the networks was invite only. Doctors’ offices would say, truthfully to the best of their knowledge that “they took all UPMC products….” And they did, they signed every contract ever offered to them. They just were not offered every contract in the portfolio.
means are the ends
@Fred Fnord Yes, California does have regulations about this, and people can file grievances and/or contact the California Insurance Commissioner about directory problems. There have been significant fines levied, but of course this is an ongoing issue. I give this info out regularly, as I work on a Mental Health Access line for a large CA county (there’s one in every county here), with our goal being to connect people to appropriate services based on their insurance. We directly administer Medi/Cal mental health services for our county, and refer out otherwise. Our provider directory is updated every day, and it takes time, effort, and money, just as stated. However, when I make a referral, it is to an active provider taking clients at that moment.
My heart sinks regularly during calls from folks with Medi/Care only, as the directory is a complete disaster. My group has resorted to actually keeping a small list of active Medi/Care referrals which we took our own time to confirm a year or so ago, just to have something to recommend to this vulnerable group of consumers, with the proviso that we have no connection with Medi/Care, and no authority to refer. Nor do we have information more updated than the directory otherwise.
These callers are most often older folks with mental health challenges trying to locate a psychiatrist, most of which are not actually available for numerous reasons. A plot twist: some of the listed psychiatrists DO take Medi/Care but are part of the county clinic system, so they take Medi/Care, but are not in private practice. You can’t just phone them up for an appt, and people keep calling us in frustration after trying to contact them.
Your tax dollars at work, btw. Thanks everyone! And sorry for going on and on!
Ms. Kate
It’s an insanely frustrating process. I just moved to an area where there are plenty of doctors (yay!). As I was checking various Medicare Advantage plans, some had as few as 5 rheumatologists, and they were 15 miles away from me. Is the info incorrect? Or is the plan that restricted? Who knows!
The better interactions where with companies who had an online portal showing the covered doctors. There was a lot more info there, and so far, it seems to be reasonably accurate. Those were plans associated with big medical groups like Kaiser and Sutter Health, that have many facilities with many providers.