The Kaiser Family Foundation is recapping the Medicare Advantage landscape files for 2019. The recap differs in details but is similar to previous years as Medicare Advantage is a well functioning program that seems to be delivering good value to both beneficiaries and the federal government.
Medicare Advantage are plans that are offered by private insurers to replace the traditional Medicare benefit package. People can buy a Medicare Advantage plan or they can stay in traditional Medicare with the option of buying a supplemental plan to provide catastrophic risk protection. Medicare Advantage is growing in popularity.
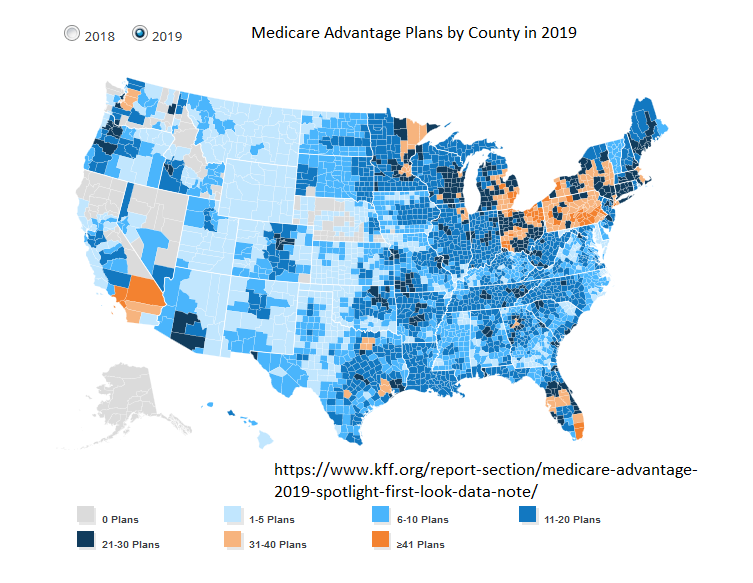
However it is not offered everywhere
No Medicare Advantage plans will be offered in 115 counties in 2019, down from 149 counties in 2018; these counties account for one percent of beneficiaries, most of whom live in relatively rural areas in California. Eight other states also have counties in which no Medicare Advantage plans will be offered in 2019 (AK, CO, IA, ID, NE, NV, VA, and WA).
And even where it is is offered, there may be low competition as a “plan” is only a single policy like a Gold $2,500 deductible narrow network is a single plan from a single insurer. A one plan county is a single insurer county.
 And very few people care.
And very few people care.
Indifference is rational as everyone who is Medicare eligible has access to baseline coverage through traditional Medicare. It is the public option of the system that acts as a backstop to the added-on layer of Medicare Advantage. It is the default that is everywhere for everyone. Some people opt out of the default but it is always there no matter strategic decisions an insurer makes due to policy, actuarial or political pressures.
ThresherK
The color range on the map is non-intuitive. Odd from the Kaiser Foundation.
WereBear
Our own experience with Mr WereBear’s Medicare Advantage is that IT SUCKS.
They demand certain tests which are optional and will upset his delicate endocrine/electrolyte balance. They call the pharmacist to jiggle with his tricky meds which took years to get to an optimal state. They send him letters declaring they have made appointments for him with doctors far away and we have to cancel them. They turn down permission for tests he does need. And when he does have a procedure, there’s all kinds of things they don’t cover.
Don’t ever get chronically ill in the US. You will be hunted to your grave.
Lucy Finn-Smith
Please be aware that Medicare Advantage ,( how were they allowed to use THAT name by the way ?) has MANY restrictions and NETWORKS. You are handing over your power ( your Medicare ) to a profit making network that is luring you in with gym offers and vision and dental care. My husband tried it for a year , couldn’t see the doctors he wanted to see, had some procedures and ended up being billed for thousands of dollars because of “out of network ” services! ( it got sorted out in the end but VERY frustrating ) , He went back to TRADITIONAL MEDICARE ( and you only get ONE chance to revert back to trad medicare )
Medicare Advantage is a SCAM in my opinion .
Butter Emails!!!
I thought Medicare advantage often had policies that were overpriced and often under-delivered compared to vanilla Medicare. Has that changed?
Yellowdog
I have Kaiser Advantage and it is great. Three dollars per presciption, five dollars copay per visit, several after hours care centers in the area. My mother had Kaiser for her last illness, which involved brain surgery and several weeks in intensive care. The only bill I got was for the ambulance that took her to the hospital.
David Anderson
@Butter Emails!!!: Over the past 5-10 years Medicare Advantage payment advantage over traditional Medicare has been mostly erased. The recent literature strongly suggests that Medicare Advantage on net delivers either equal or better total value than traditional Medicare.
in the 2000s, Medicare Advantage was a blackhole of suck.
Butter Emails!!!
OK. Thanks for the update.
PST
@David Anderson:
That would be a great subject for exploration in detail here. Many of us jackals aren’t getting any younger. I just turned 65 and went traditional, but I may have been overly influenced by obsolete information. Mostly, I worried that Advantage would be a lobster pot I couldn’t get out of if later at a reasonable cost I needed the unfettered accessibility of Medicare plus supplement. I would be interested in some kind of decision tree with variables like medical history, location, and finances that would make the choice easier. I would have been more open to Advantage if I lived in Kaiser country and felt sure I’d never move.
JaneE
Not only do rural Californians not have Medicare Advantage, some of the doctors here were still refusing to process Medicare paperwork less than 5 years ago. It’s apparently a mark of honor for GOP doctors to avoid any trace of socialized medicine, and if the patients they have been treating all their lives get old enough for medicare, they stop handling their insurance. Private insurance forms, no problem. Medicare forms, – here’s the bill, take care of the reimbursement yourself.
Barbara
@David Anderson: It was such a black hole of suck that they changed the name! The main advantage that MA has over the traditional fee for service program is that they save money by integrating care. Yes, that means they say no more often, whereas, Medicare FFS never says no. If you are a very savvy consumer who has close relationships with a doctor who is part of an organized system, whether an ACO or a very large multispecialty group, you can probably get a reasonably close facsimile of what the best MA plans try to deliver. But for most beneficiaries, the traditional Medicare program is fragmented and involves a lot of duplication and cost sharing, or else paying additional premiums for supplemental and drug coverage. My mother really liked her MA plan, which was through Coventry and then Aetna.
Barbara
@JaneE:
That’s actually illegal. They are required to submit the bill on your behalf.
David Anderson
@PST: My parents just turned 65 and they chose traditional Medicare plus a supplement as they wanted access to Mass General and anything up and down the East Coast during their “visit the grandkids” drives.
Barbara
@PST: Opting in to the traditional program is a perfectly defensible action when you don’t feel like you have adequate information about the alternatives. Your expenses are likely to be lowest at the beginning of retirement. However, for purposes of buying a Medicare Supplement plan, if you don’t buy one within the first six months (it might be a year) you will be subject to underwriting if you change your mind and buy one later. Whereas, if you immediately enroll in MA and then disenroll later, you still have a window for non-underwritten Medicare Supplemental coverage. It’s just ridiculous that this is all so complicated.
Barbara
@David Anderson: It’s funny that people have such determined views on quality. I have a well-informed acquaintance who shall be nameless who told me that they would stay out of Mass General for anything that Mass General was not uniquely equipped to deliver because they considered it to be a black hole for anything else — not worth the added expense and aggravation. Studies of value among academic medical centers provide a certain amount of support for that view. I think my views on the impossibility of judging quality among medical institutions are well-known.
p.a.
I thought the original MA, a rethug design, was a disaster that got straightened out by- surprise surprise- one of the Dem congresses of the recent past.
Mudbrush
Yeah, you can offer a lot of value for one’s healthcare dollar if you are fleecing the federal government. We will never be free of the parasitical health insurance companies. Never. They have too much money and our leaders are too easily corrupted.
Barbara
@p.a.: There have been multiple iterations of Medicare risk plans. The current design, with private bidding, went live in 2006. Congress threw a lot of money at them and began withdrawing the surplus funding in 2008, effective beginning 2010. That transition ended in 2017 (although most plans were at or below FFS actuarial equivalent by around 2014). Oversight by CMS has been basically apolitical, that is constant over the course of time no matter who has been in charge of the executive branch.
The political problem with Medicare Advantage at the beginning of the program is that a lot of senators and congressional reps were adamant that every senior have access to an MA “alternative” even in those counties where, basically, it’s impossible to establish a private plan unless you throw a lot of money at the “problem,” which they did. There were also a lot of Republican pet rock ideas thrown in, such as MSAs and something called PFFS plans. All of that has basically been washed out over time, although I think the latest funding was more generous than expected.
Barbara
@Mudbrush: The reality is that “for-profit” healthcare companies permeate both provider and payer elements. Realizing that it’s not always easy to figure out what constitutes overutilization, MA plans tend to have much lower utilization of certain types of high cost resources, and reserve them for cases where they are more clearly necessary. I can’t say too much about this, but the picture is gray — nearly everyone in all positions along the spectrum of health care have their share of greed and good intentions. Part D plans that are integrated with MA plans tend to be more generous than those offered by standalone Part D plans, because MA plans can better integrate drug and medical care. Fragmentation — especially at transition points — is a huge problem in the fee for service program. It’s much less of a problem in MA plans.
Michael Cain
@JaneE: “…some of the doctors here were still refusing to process Medicare paperwork less than 5 years ago.”
We still have rural areas where there are no doctors that accept new Medicare patients. One of the differences between “single payer” as used in most of the world and in the US is that outside the US the docs usually don’t have a choice. Unless they’re going to run a concierge practice for the wealthy, they have to accept insured patients. All the medical insurance in the world is worthless if the providers won’t accept it.
bt
What is the story with Pennsylvania I must ask?
David Anderson
@bt: I don’t know. I am guessing that the market structure of a significant number of local 600 pound gorillas plus a very old population probably matters.