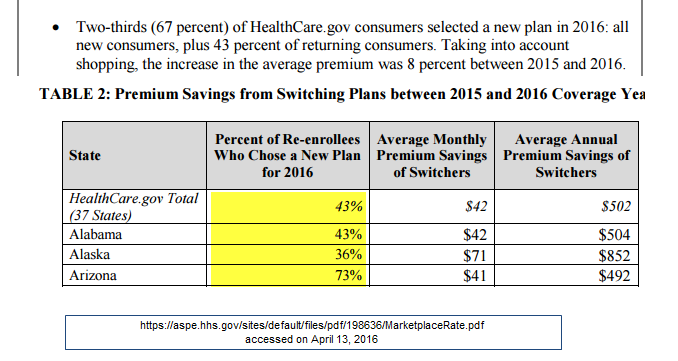
Healthcare.gov and the Health and Human Service (HHS) research group ASPE just released a summary of the shopping tendencies during the 2016 Open Enrollment Period for Healthcare.gov states. There are lots of very interesting nuggets in it, but one table leaped out at me as it plays to my hobby horse of churn analysis:
How the hell do you do population health management on a population that is this transient***?
The short answer is you really don’t.
The long answer is that it is complicated. The stickers are more likely to be sick than the switchers so there is some value of population health management for the people who are actually sick and driving the expenses. But realistically, the Exchanges make up 4% of the US population. The individual market has historically been a high churn market where people stay in it until something better comes along. The Exchange market is similar to the pre-Exchange individual market in that aspect. The population health management focus of the ACA is far better targeted at the Medicare population as Medicare is where the probability of chronic conditions (ie being old) is very high over a very large population. That market has a good bit of churn but it also has mature risk adjustment systems in place with experienced players. Insurers will still see a good amount of churn but the process smooths it out plus the benefits of active population health management are fare more likely to be at least a break even proposition for the insurer in any given year.
*** I have a question into ASPE if they are including people who move from 2015 Mayhew Silver HMO to 2016 Mayhew Silver Narrow EPO in the mover category? I think they are. If that type of movement is being accounted for, the population is not quite as transient as the population health manager for Mayhew Silver Narrow EPO sits on the bathroom side of the 13th floor and the population health managers for Mayhew Silver HMO sit next to the kitchen on the 13th floor.
p.a.
Sorry to go OT but don’t want to wait for an open thread. If you’re in the Northeast and you see a group of my former Vz coworkers picketing give em a few taps of the horn to show your support. It really will be appreciated.
Linnaeus
@p.a.:
As one who has walked a picket line or two, I second this.
Major Major Major Major
Hey Richard, I just wanted to say that I really appreciate your posts about this stuff even though I don’t comment. (I tend to read them in tranches.)
p.a.
And it’s not really that ACA OT: their health ins ends at 4/30. As a retiree we still don’t know our status.
Richard Mayhew
@p.a.: Amen, solidarity….
Also the ACA helps out the CWA for if they lose their coverage on 4/30, a Special Enrollment Period triggers for 5/1
https://balloon-juice.com/2015/08/03/labor-capital-disputes-and-the-aca/
jl
Switzerland has shown that a health system based mostly on private insurance can have low churn rates. I think much less than 10 percent. (Edit: I think recently, it is down near 5 percent per year.)
But, they have a system where it was possible to destroy networks and create provider markets with relatively transparent pricing and quality.
And soft price control insurance premium and provider service charge bands, backed by open-book audits for those who deem themselves very special and deserving of more loot than others.
I don’t think Swiss mechanisms to achieve those ends are feasible in the US. Industry wide cartelized negotiations over provider fees for services cannot be directly transplanted to the US, for example. But my motto is destroy all networks and destroy all local monopoly and oligopoly pricing.
If we continue down PPACA route, those need to be the next goals.
And neither HRC nor Sanders really tackles those issues. Sanders wants a magical leap into the politically impossible (in the near term at least), without a word about what do in the meantime. And HRC’s plan is way to small bore micro-tweaking, while insisting that all is basically well with PPACA. I think too many are too unhappy with continuation of overly costly care for that to be a compelling program.
amygdala
Interesting article in today’s New England Journal of Medicine on ACOs in the first couple of years of the ACA. It’s full-text access, even.
The whole issue is pretty interesting, with a piece on the serious unlikelihood of single payer in the US, a clinical trial in which fusion didn’t add benefit to decompressive laminectomy for spinal stenosis (this could save $$), and the establishment of a link between Zika and microcephaly. And those are all full-text.
Draftmama
Please tell someone the new format of this website sucks. I have always enjoyed reading it but it’s now off my bookmarks. Pretty pathetic. Formatting.